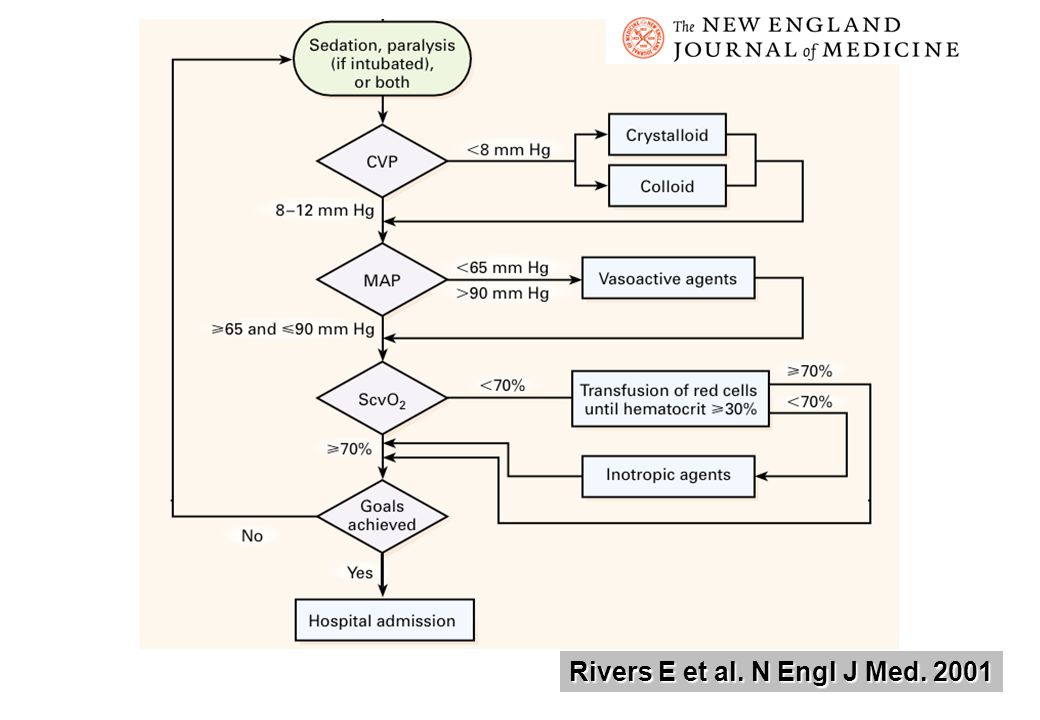
As per the Rivers E et al. study, EGDT decreased short term mortality and many non randomized before and after studies reported survival benefit despite its incomplete or partial implementation. In 2004 the Surviving Sepsis Campaign guidelines endorsed EGDT.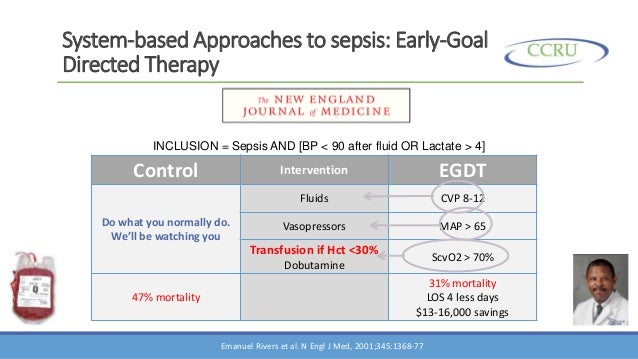
However recently three large multicentre RCTs' the ARISE, ProCESS and ProMISe failed to demonstrate any decrease in mortality following EGDT.
This was studied in "A systematic review and meta-analysis of EGDT for Septic Shock: the ARISE, ProCESS and ProMISe investigators" by D C Angus et al.
This group has concluded that EGDT is not superior to usual care for ED patients with septic shock and in fact increases utilization of ICU resources in the form of increased ICU admissions and vasopressor use.
The authors do not support the use of EGDT in management of all patients of septic shock or its inclusion in Surviving Sepsis Campaign.
To read more on this please follow the link below:



 To read more about this please follow the link
To read more about this please follow the link